
- Facelift
- Eye
- Eyelid Revision
- - Cause of depressed scar and eyelash eversion
- - Pretarsal fullness “Sausage deformity”
- - Triple folds (Multifolds)
- - Shape of double eyelid
- - Epicanthoplasty revision
- Primary double eyelid surgery Nonincision Partial-incision, incision
- - Primary Double Eyelid Procedure
- - Non-incision & Partial incision Suture ligation technique for double eyelid folding/ Non-incisional Blepharoptosis correction
- - Incisional Blepharoplasty procedure
- Epicanthoplasty lateral canthotopy lower traction
- - Epicanthoplasty
- - Lateral Canthotomy and canthoplasty outside further opening
- - Lowerlid traction
- Blepharoptosis Correction/Eye opening enhancement
- Eye bag, Transconjunctival blepharoplasty, Midface enhancement
- For Middle Age
- - Sagging eye
- - Lower Blepharoplasty
- Eye surgery Notices
- Nose
- Nose reoperation
- Low Nose
- - Low Nose Surgery
- - Reduce nose (Osteotomy)
- Male Rhinoplasty
- Artecoll Nose Surgery
- Nose tip surgery
- Wing of nose surgery
- Short nose, long nose
- Columella plasty
- Hump Nose deformity, Aquiline nose
- Corrective Rhinoplasty for Crooked Nose, Nasal Septal Deviation
- Nostril Reduction
- Rhinoplasty Notices
- Facial contouring
- Breast / Body contour
- Breast enlargement surgery
- - Drop-shaped Breast Surgery
- - Circular Breast Surgery
- - Fat Grafting Breast Surgery
- Breast reduction surgery
- Drooping breast correction
- Nipple Surgery
- Gynecomastia
- Polymastia
- Breast Restoration Surgery
- Breast reoperation
- Breast surgery Notices
- Double S Line
- Liposuction
- Abdominal Plastic
- Hip-up Surgery
- Calf Plastic Surgery
- Accusculpt
- Body Shape Injections
- Hair
- Mesotherapy & etc.




- 홈으로
- Eyelids
- Non-incision & Partial incision Suture ligation technique for double eyelid folding/ Non-incisional Blepharoptosis correction
| Duration of procedure It takes less than 30 minutes |
Anesthesia Local anesthesia with light sedation |
Hospitalization None |
No stitch to remove when non-incision/ 3days after Partial incision | Recovery Period Normal activities after 2 days, 70% of swelling fade away within 7days |
Additional to our stitching method, looping helps disperse the eye’s effort to resist the double eyelids, making it more difficult to return back to your eyes.
Since JJ 10 point non-incision method is done with small holes, the outcome looks more natural with less scars.
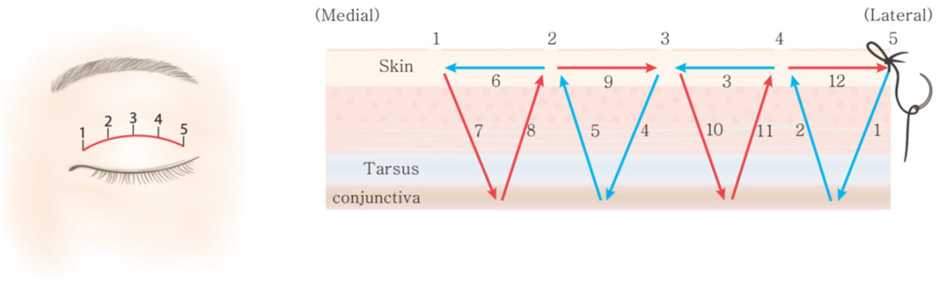
JJ 10 point non-incision suture method makes five identical loops on the eyelids. A single loop or stitch might have faster recovery periods but they tend to get loose easily. With five balanced loops that we make, your double eyelids becomes stable.
A double eyelid line should be designed along the natural skin creases on the skin of the lid. Even in a simple non-incision technique, irregularity can be happen by the undesirable design.
For a puffy eyelid, the septal fat should be removed through small incision on the double eyelid line before suture ligation procedure. Partial-incision technique means suture ligation method with the septal fat removal.

From Ch 12 Double-Eyelid Surgery :
Nonincisional Suture Techniques p 161Aesthetic Plastic Surgery of the East Asian Face, 2016 Thieme Written by Dr Jin Joo Hong and Hae Won Yang
Traditionally, the procedure can be divided into two major categories: nonincisional suture ligation (buried suture technique) and the external-incision technique. While the nonincisional technique connects the skin and the deeper active levator mechanism with a simple thread loop, the external-incision technique consists of reducing the volume of both lamellae and fixing them together with scar adhesion. The external-incision technique also requires a buried suture to connect the skin and levator mechanism, so a suture loop ligation is common to both techniques. Regardless of the use of an incision, a buried suture loop in the lid is an essential part of double-eyelid creation. In fact, the nonincision suture ligation technique entails forming a fold with suture ligation without dissection. Various surgi¬cal approaches for nonincisional suture ligation have been reported. The nonincision suture ligation technique has been developed for correction of blepharoptosis as well as for the simple formation of the double-eyelid fold. From the conjunctival side, the retractor can be plicated to increase the tension of the levator mechanism.
In the unilateral or bilateral mild ptosis case, transconjunc¬tival Müller tucking can be done with the double-eyelid operation. The preoperative design of the dou¬ble fold line should be performed along the natural skin crease. The locations of Müller tucking sutures are marked on the vertical line of the medial and lateral limbi. The sur¬gical procedure is usually performed under local anesthesia using 2% lidocaine mixed with 1/100,000 epinephrine and mild intravenous sedation. Small incisions are made with a needle or no. 11 blade on points that the needle would penetrate. Everting the upper lid, a traction suture is made on the upper margin of the tarsus with nylon 5–0.
For Müller muscle tucking, 7–0 nylon thread is intro¬duced through the skin to the upper margin of the tarsus. The suture is passed through the tarsus to the point of the conjunctiva near the superior fornix and returned through the same point on the conjunctiva to the tarsus, tucking the Müller muscle. The suture exits through the tarsus to the skin and is knotted to tighten the thread. The same proce¬dure should be performed at other sites of Müller muscle tucking, and then the traction suture is removed. Next, the common procedure for the double fold is performed. The knots of the threads should be buried within the skin so that they are not exposed.
quick menu open
-
Operating hours
- Weekdays
- 09:30~19:00
- Saturdays
- 09:30~17:30
- break time
- 12:00~13:00
-
Tel.
(+82)2.544.8807


